Pediatric BRUE (Brief Resolved Unexplained Event): What PAs Should Know

You are a physician assistant working a shift in the pediatric emergency department when EMS calls in a report of a 6 month old who turned blue and was unresponsive for 30 seconds at home. By the time they arrived the baby looked well, they transported to your facility for further evaluation. The baby is cooing, and smiling, vitals are stable and the parents are horrified. You wonder, in a well appearing infant, how far down the rabbit hole do you really need to go?
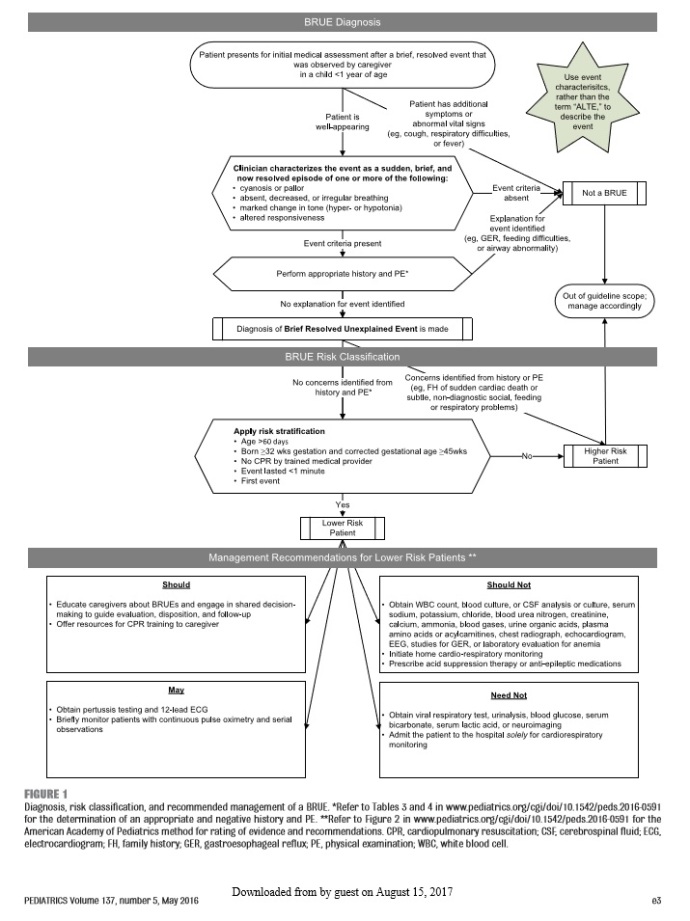
The AAP (American Academy of Pediatrics) published an article titled BRUE (Brief Resolved Unexplained Event) which changed the language we used to use for infants with an “episode” which we could not define. The guideline essentially replaced the former term “Apparent Life Threatening Event” (ALTE), with a simpler definition. I, for one, love algorithms (when used properly), so I was excited to review this one.
Pros:
-The algorithm clearly highlights age requirements (>60 days and <1 year), also reveals that the patient must be well appearing, episode cannot be explained and defines event criteria. (although a con is that this means a choking episode or reflux is not technically a BRUE has it had been called an ALTE in the past)
-the workup is limited if patient falls into the low risk category (which is what we’d like to do many times), and you are supported by the evidence.
 AAP BRUE Guideline
AAP BRUE Guideline
Cons:
-If the patient falls into a “higher risk” box there is no real guidance on management.
-It does not really help a provider work through the differentials such as abuse or other trauma, seizures, metabolic disturbances.
-there is no clear answer to which physical finding would be considered “concerning”. Is a murmur or sacral dimple concerning? There is a long list of physical exam features but it is cumbersome to say the least.
-some of their evidence for things such as the use of a pulse ox is a grade D recommendation (weak) which is lower than a standard of care. The grade C (moderate) suggestions are not to perform CT brain or UA, which also makes me a little uncomfortable since UTIs that go untreated can lead to septic infants and abuse cases that aren’t picked up are devastating in all regards.
Bottom Line:
Overall my opinion is that the guideline is helpful for those low risk patients, but relies heavily on practitioner experience- which leaves students and novices at a large disadvantage. Clinically it can be difficult to hear a murmur with a heart rate in the 130s if you don’t see them often, and a novice physician assistant may not pick up on the social nuances that come with the possibility for abuse.

PA Pearls of wisdom:
-Get a good history of the event, have the parent “paint a picture” of exactly what happened. Ask for specifics:
- How long was the event?
- What exactly occurred?
- Was there any color change? Red or blue?
- Did the patient stop breathing? For how long?
- Was the patient unresponsive? Did they do anything to try and wake them?
- Was there loss of tone or increased tone? Any shaking?
- How long from a feeding did this occur?
- Who are the primary caregivers? Parents? Grandparents? Babysitters?
- Any recent illnesses, fevers or congestion?
-Birth history is important: prenatal care, age of gestation, GBS status and treatment, maternal history of STD, drug or alcohol use
-Family history is important, ask the parents about sibling deaths, sudden deaths in the family.
-Social history is also important, if there is any social concern, the patient no longer meets “low risk”
-Do a thorough physical exam, a VERY thorough exam.
- Make sure the patient is gowned or at least down to a diaper.
- Palpate every inch of the patient’s skull
- Listen for murmurs, for as long as you need.
- Check for petechiae
- Look for signs of injury (frenulum tears, bruising, tenderness on exam)
- Look for mottling, delay in cap refill
- Check red reflexes
- This is the most important time to be thorough- if the baby were to come back tomorrow with a bad outcome, do you feel confident that you haven’t missed anything?
-When in doubt, talk to your supervising physician. Part of being a good physician assistant is knowing who your high risk patients are, and a new provider may need to lean on more experience to help navigate through the decision tree
Overall, I hope this helps you think about how to manage these patients. I prefer a systematic approach when it comes to ambiguous diagnoses, hopefully this gives you a place to start!
C
If you enjoyed this, consider following EmpoweredPAs.com on social media links below, or sign up to our email list for more great content addressing topics about evidence-based practice, PA time management, leadership skills, pediatric emergency medicine tips, Pre-PA action plans, PA Student study tips, free resources such as PDFs and ebooks.
 Next Post
Next Post