Rapid Strep Tests in Kids- Can You Apply Centor Criteria?


Ah, Strep. The “bread and butter” diagnosis of urgent care, ER and primary medicine.
As a PA, do you use the Centor Criteria to treat “Strep throat”? Do you “always” perform a rapid strep test to make a treatment decision? If so, do you also obtain a strep culture? Do you use evidence based methods or local consensus?
Strep pharyngitis, which is also referred to as GAS (Group A Strep) , GABHS (Group A Beta-Hemolytic Streptococcus) is commonly diagnosed by Physician Assistants in clinics and hospitals world wide. According to the CDC, viruses cause most cases of pharyngitis, with GABHS only causing up to 30% of pharyngitis in children and up to 15% in adults. Complications include scarlet fever, acute rheumatic fever, post strep glomerulonephritis, and pharyngeal abscesses. It can also trigger Kawasaki Disease (which, by the way, should concern you in a big way if the patient looks clinically ill or toxic).
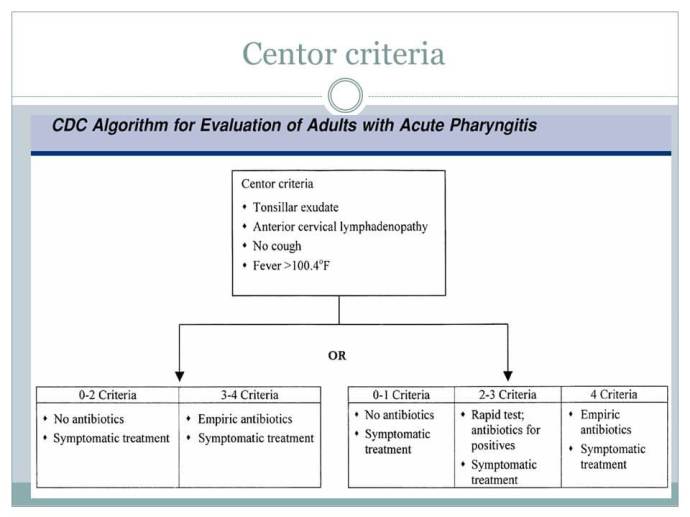
Because viruses are more likely to be the cause, studies were done to help decide when to use the rapid strep test. The most commonly known (at least in my part of the world) is the Centor criteria.
The original study was in 1981 by Robert Centor, with an age modification by McIssac group in 1998, and 2004, and an update by Harris et al in 2016. It suggested a point scoring system which was eventually modified by McIssac for age:
However…
Robert Centor himself, noted it’s pitfalls when applied to children. He said, on MD Calc Centor Score:
What pearls, pitfalls and/or tips do you have for users of the Centor Score? Are there cases when it has been applied, interpreted, or used inappropriately?
We studied adults, and thus have always been wary of applying it to children. More recently, we have published a review that shows that pre-adolescent pharyngitis has many differences from adolescent/young adult pharyngitis. McIsaac has developed an adjustment for age which might be appropriate for pre-adolescents.Please do not use this score if the patient does not have a recent onset acute pharyngitis (3 days or less). Some have erred in using this for any throat discomfort.
The McIssac 2004 Validation study did support the importance of sending off a strep culture if a rapid strep is negative in children (not so much in adults). It also suggested, on my interpretation of table 5 that you really cant apply the same plan of action to pediatrics. When they applied the “perform rapid strep followed by culture” plan to adults, there was 0 call backs, but when kids had negative rapid strep tests, 22 patients had positive cultures. For clarity they do say you can apply the modified criteria to pediatrics- I disagree.
Why I always test pediatric patients over age two:
The British Medical Journal published a study (BMJ Study of Centor Criteria for Strep Pharyngitis) was a retrospective study looking back over the charts of over 400 pediatric patients age 2-16, and suggested that Centor criteria was not predictive of GABHS in children.
AHA- Prevention of Rheumatic Fever.. (2009)– suggests that a clinical algorithm may be acceptable in adults but not children, and stresses my concerns that the approach could result in a large number of patients being inappropriately prescribed antibiotics.
I will note that Fine et al (2012) study was a huge (>200,000 patient) retrospective study over 3 years from a “minute clinic” setting- and essentially validated the Centor and McIssac studies, though I can’t completely be sure of the bias.
So- what does the Empowered PA do?
You should treat based on your level of comfort your supervising physician, and I always suggest using evidence based practice (see the above).
On that note, I work in a pediatric ER setting.
- If there is any suspicion (palatal petechiae, fever, exudates) I will perform a rapid strep over age 2 (I make sure to obtain the swab, so I know it is accurate).
- I only treat if positive and if negative then a culture is sent for confirmation, and I tell the family we will contact them if the culture is positive.
- I keep in mind that pediatric patients are sometimes carriers of strep and my practice is not to swab unless there are clinical symptoms to support the test.
- Make sure to document no signs of pharyngeal abscess (no uvular shift, no asymmetry, normal neck ROM), and that you do not suspect kawasaki disease (no conjunctival injection, desquamating rash etc).
- I also (try to) educate families to watch for hematuria and post strep GN if there was a delay to antibiotic treatment.
But what about under 2 years old?
The answer is complicated, but CDC and multiple resources mention that there is little indication to test the average healthy patient under age two. This is mostly because patients under two years old are not shown to develop rheumatic fever. The caveat to that is if the patient is at higher risk for GABHS infection (sibling has active infection, immunocompromised etc). The direct answer is, it’s not supported in the literature, and is costly, but may be indicated in higher risk populations.

Treatment Pearls
- remember you can treat with amoxicillin once daily for strep! (this is not the case for pneumonia or otitis)
CDC Dosing for acute Group A Beta-hemolytic Streptococcal Pharyngitis:
| Drug, Route | Dose or Dosage | Duration or Quantity | |
|---|---|---|---|
| For individuals without penicillin allergy | |||
| Penicillin V, oral | Children: 250 mg twice daily or 3 times daily; adolescents and adults: 250 mg 4 times daily or 500 mg twice daily | 10 days | |
| Amoxicillin, oral | 50 mg/kg once daily (max = 1000 mg); alternate:25 mg/kg (max = 500 mg) twice daily | 10 days | |
| Benzathine penicillin G, intramuscular | <27 kg: 600 000 U; ≥27 kg: 1 200 000 U | 1 dose | |
| For individuals with penicillin allergy | |||
| Cephalexin,a oral | 20 mg/kg/dose twice daily (max = 500 mg/dose) | 10 days | |
| Cefadroxil,a oral | 30 mg/kg once daily (max = 1 g) | 10 days | |
| Clindamycin, oral | 7 mg/kg/dose 3 times daily (max = 300 mg/dose) | 10 days | |
| Azithromycin,b oral | 12 mg/kg once daily (max = 500 mg) | 5 days | |
| Clarithromycinb, oral | 7.5 mg/kg/dose twice daily (max = 250 mg/dose) | 10 days | |
-C
If you enjoyed this, consider following EmpoweredPAs.com on social media links below, or sign up to our email list for more great content addressing topics about evidence-based practice, PA time management, leadership skills, pediatric emergency medicine tips, Pre-PA action plans, PA Student study tips, and other resources such as PA School spreadsheets, patient logs, PDFs, and ebooks.
